by Christo Lues
What is an un-natural pregnancy
Well as you’ve probably guessed by now, an un-natural pregnancy is more or less the opposite of what you have read in Part 1. Unnatural pregnancy is where unnecessary intervention is allowed by the mother or taken by a medical professional, deeming the natural flow of pregnancy or birth ineffective or dangerous.
In this case the mother will suspect that she is pregnant, because she has just recently come off a contraceptive and has missed her expected monthly cycle. She may do a home pregnancy test, but will not trust it, so she pops down to the doctor to have it confirmed by an expert. The doctor will prescribe folic acid and may tell her that nothing else (like vitamins and herbs) should be taken during pregnancy, as this can be dangerous - folic acid is all that is needed…
From the GP, the mother will go to a gynaecologist for more ‘professional assistance’ during her pregnancy. The assault on the infant begins with the invasive ultrasound. In order to check that everything is on track, the gynaecologist will do regular ultrasound scans, from as early as 6 or 8 weeks. Every time the mother visits the doctor he will do an ultrasound and may even do internal/vaginal examinations to ‘check’ if she is doing OK.
 In 2004 the FDA warned: "ultrasound is a form of energy, and even at low levels, laboratory studies have shown it can produce physical effect in tissue, such as jarring vibrations and a rise in temperature." These temperature increases can cause birth defects and result in central nervous system damage. A large randomized trial conducted by the RADIUS Study Group found the use of ultrasound did not result in improved outcome in pregnancies.
In 2004 the FDA warned: "ultrasound is a form of energy, and even at low levels, laboratory studies have shown it can produce physical effect in tissue, such as jarring vibrations and a rise in temperature." These temperature increases can cause birth defects and result in central nervous system damage. A large randomized trial conducted by the RADIUS Study Group found the use of ultrasound did not result in improved outcome in pregnancies.
Learn more here...
Because of the internal examination the mother may have bleeding the same day or the next day. Because she is really concerned, she will phone the doctor and explain the bleeding. The doctor will want to see her and may do another ultrasound scan or a follow-up internal examination to see if there is any problem. If the baby is still alive after this poking and video game session the bleeding may stop after a day or two.
It may also happen that because of her higher progesterone levels that the young lady has an elevated sexual desire, leading to more frequent intercourse. Because her body goes through many hormonal changes, her vaginal wall may be richer in blood supply and during intercourse some of the tiny delicate blood vessels may naturally rupture, resulting in light pink discharge.
When she discovers this the next morning, the above doctor procedure will possibly be repeated.
The gynaecologist will suggest various tests to be carried out on the unborn baby and the mother. One of which is an amniocentesis.
Wikipedia: Amniocentesis (also referred to as amniotic fluid test or AFT) is a medical procedure used in prenatal diagnosis of chromosomal abnormalities and fetal infections, in which a small amount of amniotic fluid, which contains fetal tissues, is sampled from the amnion or amniotic sac surrounding a developing fetus, and the fetal DNA is examined for genetic abnormalities.
This will show a (statistical) possibility of Downs syndrome. Apart from the fact that many NORMAL pregnancies (babies) have been terminated (murdered) by the actions following the inaccuracy of the test, it carries many other known risks:
Wikipedia: Amniocentesis is performed between the 15th and 20th week of pregnancy; performing this test earlier may result in fetal injury.[8] The term "early amniocentesis" is sometimes used to describe use of the process between weeks 11 and 13.[9]
Complications of amniocentesis include preterm labor and delivery, respiratory distress, postural deformities, fetal trauma and alloimmunisation of the mother (rhesus disease). Studies from the 1970s originally estimated the risk of amniocentesis-related miscarriage at around 1 in 200 (0.5%).[10] Three more recent studies from 2000-2006 estimated the procedure-related pregnancy loss at 0.6-0.86%. [11] A more recent study (2006) has indicated this may actually be much lower, perhaps as low as 1 in 1,600 (0.06%). [12]. Unlike the previous studies, the number in this study only reflects the loss that resulted from amniocentesis complications and excluded the cases when parents decided for an abortion following the test results.[11] In contrast to amniocentesis, the risk of miscarriage from chorionic villus sampling (CVS) is believed to be approximately 1 in 100, although CVS may be done up to four weeks earlier, and may be preferable if the possibility of genetic defects is thought to be higher.[13]Amniotic fluid embolism has been described as a possible risk.

If none of the above happens and the brave mother decides to keep the (possibly) Downs baby, she may be overcome with worry, fear and uncertainty for the rest of the remaining pregnancy, stealing her joy of being pregnant. It should be stated that before doing the test, you should think through what you will do with the (mostly inaccurate) results, after the test is done. Put differently, if you are pro life, what is your rational for doing a test to tell you whether your baby is normal or abnormal and should be aborted.
On paper this looks really simple, but it is an entirely different scenario that plays off in the doctor’s rooms. The mother may be put under so much pressure by the ‘well meaning’ doctor that she will give in to doing the test, possibly resulting in one or more of the above (fatal for the baby) side effects.
I have seen a mother literally go insane after she struggled to fall pregnant for many years, then fell pregnant, only to abort her perfectly normal baby due to the inaccurate statistical probability of the child being Downs with the amniocentesis!
Next in line is a test the ‘caring’ doctor would like to do by taking a sample from your cervix to determine if you have some ‘dangerous’ streptococcus bacteria living in your vagina. Group B streptococci colonize the vagina, gastrointestinal tract, and the upper respiratory tract of healthy humans. It is an invasive encapsulated organism capable of producing disease in immunocompromised hosts, like any of the more or less 400 other bacteria found in the human digestive tract, vagina, mouth, throat etc. Young and middle-aged women who undergo obstetrical and gynecological manipulation are at an increased risk of group B streptococcal infection. If this is found you will be put onto strong antibiotics during labour, to ‘protect’ your baby from your dangerous vagina.
To put this in perspective, if you are a healthy woman, having a natural birth without the doctor performing unnecessary invasive procedures (that will release or disturb the Strep B) you are safe.
So lets assume that you and your unborn baby survived the numerous ultrasounds, the amniocentesis, the Strep test and any other tests or procedures your health professional conjures up, next is your regular checkups in the last trimester of pregnancy.

Nothing can go wrong from here on, right? Your doctor told you that he/she is for natural births…the problem is that the gynaecologists‘ understanding of a natural birth is probably quite different from yours. Your battle for a natural delivery, if you wished to have one has just begun!
In South Africa, if you go to a private gynaecologist, you have a 80%+ chance of getting a Caesarian section. If you are at a state hospital you have a 5% chance of getting a Caesarian section. In the UK where the NHS pays for medical costs, you have a 5% chance of getting a Caesarian section. Why? Is it because when you go private that you are more sickly or conversely healthy mothers go to state hospitals? Or is it just a matter of mothers with bigger babies go private and mothers with small babies go the government route? Does not sound logical, does it?
In general the cost of a normal delivery at a Government hospital, if you are a normal person that can pay would be around R10 000.
When you go private for a birth (95% certainty a C-section) the cost is around R40 000, depending on what hospital you attend. Compare this to around R6000 for a home birth with a midwife.
 So, do you think there may be a financial incentive for doing a c-section vs a normal delivery? Do you think there may be a financial incentive to ‘knock’ midwifes, natural births or home births? Incase you missed it YES! It’s WAY more lucrative to do a c-section than a normal delivery, and it’s way easier for a gynaecologist so ‘schedule’ your c-section into his busy program than an unpredictable normal delivery that may take many hours longer.
So, do you think there may be a financial incentive for doing a c-section vs a normal delivery? Do you think there may be a financial incentive to ‘knock’ midwifes, natural births or home births? Incase you missed it YES! It’s WAY more lucrative to do a c-section than a normal delivery, and it’s way easier for a gynaecologist so ‘schedule’ your c-section into his busy program than an unpredictable normal delivery that may take many hours longer.
So when your private gynecologist tells you he or she is PRO-natural birth, you should be aware that as your pregnancy progress, points of concern will arise that, according to your gynecologist, will make a natural birth almost impossible.
As your pregnancy develops, the gynecologist will want to see you at regular intervals to ‘check’ that everything is normal, doing more ultra sound scans and internal examinations.
His talks about a natural birth will start fading as you near the end of your pregnancy.
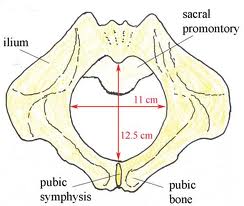
He will start using words like: “Your baby seems a bit bigger than expected” or “You have a healthy big baby, it would take some pushing to get it out” or “Lets do a pelvic estimation” this means that he guesses that your pelvis is too small and that even if you wanted to, the baby won’t fit through your pelvis.
This will leave the young and ignorant mother with seeds of doubt about a natural delivery. In time the doctor will reinforce his initial premise. He will now use words like: “Way too big” or “may get stuck” or “high risk delivery”. If the young mother is brave and dare resist him, he will change tactics. The husband is next. What husband wants to put his wife’s life in danger - none! So the gynecologist will appeal to the man’s natural sense of protection over his wife and may use words like: “Natural delivery will endanger your wife’s life, and possibly that of the baby” or “As a father you may have to make a logical choice for safety” the father will now (subtly) start siding with the doctor for the ‘safety’ of his family.

On the next visit and closer to term the doctor will use words like: “The placenta is starting to calcify and we need to act soon” or the doctor may take the exited mother’s blood pressure and find it slightly elevated. In this case he may then admit the mother to the maternity ward and start inducing the labour - to ‘save’ her life of course.
Because the baby is not ready to be born yet, the induction will usually fail, resulting in an “emergency c-section”.
It may also happen that the doctor ‘allow’ the mother to try for a natural birth, but only on his terms. This means the doctor will say: “We have your safety at heart and for that reason you absolutely cannot go past a certain time” this ‘time’ is in some cases one to two weeks before the real expected date of the baby. If the mother does not go into spontaneous labour by her ultrasound calculated expected date, a c-section is scheduled. Ultra sound scans calculate the birth date by the size of the baby and the size is just an estimation and not very accurate. The chance of the mother going into spontaneous labour is slim taking in account the stress she is now under to go into labour by a given time, and stress inhibits labour hormones - (Read more on Linnie’s BLOG), so the doctor gets his way anyway, but the mother buys the augmented truth that it was the only ‘safe’ alternative and that she had to have a c-section.

One other scenario is that the doctor allows the young mother to go into labour, but the moment it happens puts her on her back on a bed, on a fetal monitor and gives an epidural for pain free delivery. An epidural can be given for the pain - numbing the body, thereby making pushing virtually impossible. The down side is that the mother lies on her back and does not have gravity to help get baby out - a c-section may result. Alternatively an instrument delivery with an accompanying episiotomy may result - unnecessary pain for the mother and possible trauma for the baby.
There is no end to how the truth will be twisted, so it suffice to say that the “well meaning gynaecologist” will do his utmost best to get the woman in for a c-section, he profits, the hospital profits and the costs are covered by the medical aid - every body is happy.

The young mother has lost out on something wonderful that was intended for her and her baby. Some of the motivating factors why so many c-sections are performed includes fear of litigation over complications in delivery, fear of the unknown, personal schedules, simple lack of knowledge and sadly, money.
Great article. My first gynae tried a lot of excuses along the way, I luckily still ended up having a natural birth even though one of her reservations was my shoe size lol, I used midwives for my second and third natural births, my third baby being 3.9kg, and I am a 40kg 5foot woman. Gynaes really do try to pressure you into a cs, and sometimes for silly reasons. I'm grateful for midwives and try to punt them to everyone. A natural birth is possible for anyone if all goes well.
ReplyDelete